My #ASH24 takeaways
The 66th annual American Society of Hematology (ASH) meeting again did not disappoint. Approximately 30,000 people (Health care professionals, pharmaceutical representatives, researchers, and others converged on San Diego, CA, for this premier meeting. I was able to attend many key oral abstracts and education programs related to multiple myeloma. The presentations came like a firehose of information.
My “short” list of key takeaways:
Quadruplet Myeloma Therapies
Not-so-unexpected information was shared that reinforces the benefits of quad therapy in the newly diagnosed myeloma setting.Daratumumab-Based Quadruplet Versus Triplet Induction Regimens in Frontline Transplant-Eligible Newly Diagnosed Multiple Myeloma: A Systematic Review and Meta-Analysis, Abstract 258, Joao Tadeu Damian Souto Filho, MD Faculdade de Medicina de Campos, Campos dos Goytacazes, RJ, Brazil
Isatuximab, Lenalidomide, Bortezomib and Dexamethasone Induction Therapy for Transplant-Eligible Patients with Newly Diagnosed Multiple Myeloma: Final Progression-Free Survival Analysis of Part 1 of an Open-Label, Multicenter, Randomized, Phase 3 Trial (GMMG-HD7), Abstract 769, presented by Hartmut Goldschmidt, MD, Internal Medicine V, GMMG – Study Group at University Hospital Heidelberg, Heidelberg, Germany
Isatuximab, Bortezomib, Lenalidomide, and Dexamethasone (Isa-VRd) in Patients with Newly Diagnosed Multiple Myeloma (NDMM): Analyses of Minimal Residual Disease (MRD) Negativity Dynamics in the Phase 3 Imroz Study, Abstract 770, presented by Robert Z. Orlowski, MD, PhD, Department of Lymphoma & Myeloma, The University of Texas MD Anderson Cancer Center, Houston, TX
Phase 3 Randomized Study of Daratumumab (DARA) + Bortezomib, Lenalidomide and Dexamethasone (VRd) Versus Alone in Patients with Transplant-Ineligible Newly Diagnosed Multiple Myeloma or for Whom Transplant Is Not Planned As Initial Therapy: Analysis of Minimal Residual Disease in the Cepheus Trial, Abstract 362, presented by Sonja Zweegman, Department of Hematology, Amsterdam UMC, Vrije Universiteit Amsterdam, Cancer Center Amsterdam, Amsterdam, Netherlands
Final Analysis of the Randomised UK MRA Myeloma XI+ Trial Examining Krdc (carfilzomib, lenalidomide, dexamethasone and cyclophosphamide) As Induction Therapy for Newly Diagnosed Multiple Myeloma Patients, Abstract 771, presented by Charlotte Pawlyn, PhD, The Institute of Cancer Research, London, United Kingdom
Information related to real-world experience, enhancing patient quality of life, and addressing frailty continues to be highlighted at an increasing volume.
24-Hour Urine Testing Does Not Add Value to Multiple Myeloma Response Assessments: A Secondary Analysis of BMT CTN 0702, Abstract 81, presented by Rahul Banerjee, MD, FACP, University of Washington Fred Hutchinson Cancer Center, Seattle, WA
Balancing Treatment Intervals and Quality of Life in Multiple Myeloma Patients: Patient Perspectives and Recommendations, Abstract 284, presented by Anna Fleischer, Department of Internal Medicine II, University Hospital Wuerzburg, Wuerzburg, Germany
Real-World Characteristics and Outcomes in Patients with Multiple Myeloma Receiving Teclistamab Step-up Doses in Academic Vs. Community Settings, Abstract 933, presented by Adeel M Khan, MD, MS, MPH, Myeloma, Waldenstrom’s, and Amyloidosis Program, Hematologic Malignancies and Cellular Therapy Program, Simmons Comprehensive Cancer Center, UT Southwestern Medical Center, Dallas, TX
A High-Fiber Dietary Intervention (NUTRIVENTION) in Precursor Plasma Cell Disorders Improves Biomarkers of Disease and May Delay Progression to Myeloma, Abstract 671, presented by Urvi Shah, MD, Myeloma Service, Department of Medicine, Memorial Sloan Kettering Cancer Center, New York, NY
Outcomes of Frailty Subgroups Treated with Teclistamab in the Real-World: An International Myeloma Foundation Study Database Analysis, Abstract 704, presented by Hira Mian, MD, McMaster University, Hamilton, ON, Canada
Outcomes of Elderly Patients with Relapsed Refractory Multiple Myeloma (RRMM) Treated with Teclistamab: A Multicenter Study from the U.S. Multiple Myeloma Immunotherapy Consortium, Abstract 934, presented by Oren Pasvolsky, MD, The University of Texas MD Anderson Cancer Center, Houston, TX
Six-Month Resistance Training Interventions Are Associated with Improvements in Fatigue and Pain in Multiple Myeloma Patients, Abstract 705, presented by Janine M. Joseph, MS, MBA, Department of Cancer Prevention and Control, Roswell Park Comprehensive Cancer Center, Buffalo, NY
Lovesick: Examining Couples Health during Myeloma Transplant, Abstract 285, Presented by Ashley Rosko, The Ohio State University, Columbus, OH
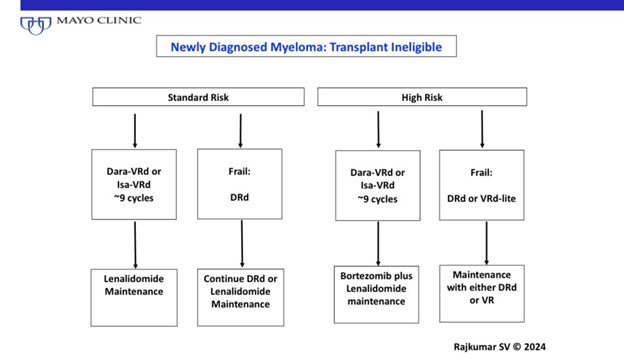
The IFM2017-03 Phase 3 Trial: A Dexamethasone Sparing-Regimen with Daratumumab and Lenalidomide for Frail Patients with Newly-Diagnosed Multiple Myeloma, Abstract 774, presented by Salomon Manier, MD, PhD, Lille University Hospital, Lille, France
Smoldering myeloma continues to be an area of controversy about whether to treat or not treat. However, results from the Aquila trial seem to be leading us in the direction of early treatment for high risk smoldering myeloma.
Phase 3 Randomized Study of Daratumumab Monotherapy Versus Active Monitoring in Patients with High-Risk Smoldering Multiple Myeloma: Primary Results of the Aquila Study, Abstract 773, presented by Meletios-Athanasios Dimopoulo, National and Kapodistrian University of Athens, Alexandra General Hospital, Athens, Greece
Longitudinal Single-Cell Immune Profiling Reveals Distinct Dynamics of Response to Teclistamab in Patients with High-Risk Smoldering Myeloma Compared to Relapsed-Refractory Multiple Myeloma, Abstract 488, presented by Nayda Bidikian, MD, Broad Institute of MIT and Harvard, Cambridge, MA
Early Safety and Efficacy of CAR-T Cell Therapy in Precursor Myeloma: Results of the CAR-PRISM Study Using Ciltacabtagene Autoleucel in High-Risk Smoldering Myeloma, Abstract 1027, presented by Omar Nadeem, MD, Center for Early Detection and Interception of Blood Cancers, Dana-Farber Cancer Institute, Boston, MA
Advances continue to be made not only in myeloma therapy, but in other domains of the myeloma experience like supportive care and identifying testing that may direct treatment decision-making
Tocilizumab Prophylaxis for Patients with Relapsed or Refractory Multiple Myeloma Treated with Teclistamab, Elranatamab or Talquetamab, Abstract 932, presented by Andrew Kowalski, PharmD, Myeloma Institute, Sylvester Comprehensive Cancer Center, University of Miami, Coral Gables, FL
Eliminating the Need for Sequential Confirmation of Response in Multiple Myeloma, Abstract 83, presented by Jean-Sébastien Claveau, MD, Division of Hematology, Mayo Clinic, Rochester, MN
Patient-Centered Care in Hematology: How Side Effect Severity Influences Decision-Making Autonomy in Relapsed Refractory Multiple Myeloma, Abstract 706, presented by Jay R. Hydren, PhD, Myeloma Service, Division of Hematologic Oncology, Department of Medicine, Memorial Sloan Kettering Cancer Center, New York, NY
A Randomized Trial Demonstrates a 3-Shot Flu Vaccine Series Improves Protection over a Single Shot in Multiple Myeloma, Abstract 255, presented by Dr. Craig Hofmiester, Winship Cancer Institute of Emory University, Atlanta, GA
Conclusion: Increased seroprotection at the end of the season by receiving three Fluzone HD vaccinations at 0, 2, and 4 months compared to a single shot.
Effects of Intravenous Immunoglobulin Supplementation (IVIG) on Infections in Recipients of Teclistamab Therapy for Multiple Myeloma (MM): A Multi-Institutional Study, Abstract 255, presented by Dr. Heloise Cheruvulath, Medical College of Wisconsin, Milwaukee, WI
Early Identification of Functional High Risk Multiple Myeloma Patients after Transplant with Diffusion-Weighted Whole-Body MRI: Predictive Role of Fat Fraction in Addition to RAC Score, Abstract 82, presented by Angelo Belotti, MD, Department of Hematology, ASST Spedali Civili di Brescia, Brescia, Italy
Total Diffusion Volume Evaluated By Whole-Body Diffusion Weighted Magnetic Resonance Image for the Assessment of Tumor Burden in Multiple Myeloma; Relations with Measurable Residual Disease Evaluated By Next-Generation Flow Cytometry and Bone Marrow CD138 Staining Assessed By Qupath, Abstract 491, presented by Kentaro Narita, M.D, Division of Hematology/Oncology, Kameda Medical Center, Kamogawa, Chiba, Japan
Circulating Tumor Cells As a Biomarker to Identify High-Risk Transplant Eligible Myeloma Patients Treated with Bortezomib, Lenalidomide and Dexamethasone with or without Daratumumab during Induction/Consolidation, and Lenalidomide with or without Daratumumab during Maintenance: Results from the Perseus Study, Abstract 487, presented by Luca Bertamini, MD, Department of Hematology, Erasmus MC Cancer Institute, Rotterdam, Netherlands
Reevaluating the IMWG Multiple Myeloma Complete Response Criterion in the Era of Mass Spectrometry: A Critical Analysis, Abstract 489, presented by Noemi Puig, PhD, Hospital Universitario de Salamanca (HUSAL), IBSAL, IBMCC (USAL-CSIC), CIBERONC, Salamanca, Spain
A Novel Prognostic System Based on Circulating Tumor Cells for Newly Diagnosed Multiple Myeloma, Abstract 490, presented by Evangelos Terpos, MD, PhD, Department of Clinical Therapeutics, National and Kapodistrian University of Athens, School of Medicine, Drosia, Attiki, Greece
Pre-Apheresis Prediction of Toxicity and Response in Patients Receiving BCMA-Directed CAR-T for Relapsed/Refractory Multiple Myeloma, Abstract 895, presented by Kai Rejeski, M, Department of Medicine III, LMU University Hospital, LMU Munich, Munich, Germany
Comprehensive Analysis of Pre-Treatment Biomarkers Associated with Toxicity and Durable Responses in Idecabtagene Vicleucel Therapy for Relapsed/Refractory Multiple Myeloma, Abstract 896, presented by Doris K. Hansen, MD, Department of Blood and Marrow Transplantation and Cellular Immunotherapy, H. Lee Moffitt Cancer Center and Research Institute, Tampa, FL
Outcomes of Teclistamab (Tec) in Patients with Relapsed/Refractory Multiple Myeloma (RRMM) with Prior Exposure to BCMA-Directed Therapy (BCMA-DT): A Multicenter Study from the U.S. Multiple Myeloma Immunotherapy Consortium, Abstract 897, presented by Danai Dima, MD, Cleveland Clinic Taussig Cancer Institute, Cleveland, OH. “Waiting >9 months between sequencing BCMA therapies may be associated with improved PFS.”
And, finally, an exciting update from the Anito-Cel trial for people with relapsed myeloma
Phase 2 Registrational Study of Anitocabtagene Autoleucel for the Treatment of Patients with Relapsed and/or Refractory Multiple Myeloma: Preliminary Results from the IMMagine-1 Trial, Abstract 1031, presented by Ciara Louise Freeman, PhD, MSc, FRCPC, MRCP, Department of Blood and Marrow Transplantation and Cellular Immunotherapy, H. Lee Moffitt Cancer Center and Research Institute, Tampa, FL
Many of these and other abstracts will be discussed in greater detail by an amazing panel of myeloma experts at the IMWG Conference Series: Making Sense of Treatment ASH 2024, being held Wednesday, 12/18/2024 at 03:00pm PST.
Dr. Joseph Mikhael, IMF Chief Medical Officer, will be joined by Beth Faiman, PhD, Nikhil Munshi, MD and Vincent Rajkumar, MD, and will discuss advances in myeloma research from the 2024 ASH Conference.
Hear the patient perspective from the Myeloma Voices who attended ASH24 as they share their insights at this webinar: Latest Myeloma Updates from ASH 2024: Easy-to-Understand Insights for Patients and Care Partners on Wednesday, 1/08/2025 03:00pm PST
These and other great events are being planned, including the 2025 Patient and Family Seminars and Regional Community Workshops. Find these and more at Myeloma.org/events.
- I want to extend my gratitude to:
- The IMF for continuing to include me in this amazing program, Myeloma Voices, where the patient voice is shared through social media to provide updates on myeloma data that impacts those living with this diagnosis. It is a privilege and an honor to attend with this group who volunteers their time to help others living with myeloma.
- Our sponsors of Myeloma Voices: Johnson & Johnson, Regeneron, and Karyopharm Therapeutics. Your support of myeloma patients’ learning is much appreciated.
- The IMF Meetings and Support Group Teams for all that you do to make this program happen. So many details that others will never know because you do it seamlessly and make it look easy.
- The Myeloma Voices, both virtual and in person. You volunteer your time, work through complex information and long schedules to attend the sessions, and share your experiences with your followers.
You can see how visible some of the leaders were at #ASH24, making the Social Media Leaderboard!

You can continue to follow these folks on social media and learn more about #ASH24 and other #myeloma happenings.
Sheri Baker @blondie1746
Yelak Biru @NorthTxMSG
Becky Bosley @MidAtlanticMSG
Barbara Davis @bkinoglu
Jessie Daw @Daw6Jessie
Oya Gilbert @HHHHFoundation
Terry Glassman @TerryGlassman
Linda Huguelet @LindaMyeloma
Teresa Miceli @IMFnurseMyeloma
Rob Salmon @salmon_rob
Jim Shoemaker @JimJhs17
Michael Tuohy @IMFmikeMYELOMA
Robin Tuohy @IMFsupport
Jenn Wieworka @jwiework
Jill Zitzewitz @JillZitzewitz
Search social media for key hashtags: #MMSM #Myeloma #ASH24 #IMFASH24
My best,
Teresa Miceli, RN BSN OCN
Myeloma Voices Nurse Liaison
Support Group Leader
IMF Nurse Leadership Board