Monday afternoon at ASH found me listening to an abstract by Nora Grieb. It was a study from the German Registry for Hematopoietic Stem Cell Transplantation and Cell Therapy. Autologous stem cell transplantation (ASCT) following high-dose chemotherapy is a standard treatment for newly diagnosed multiple myeloma patients. Tandem transplantation, involving two ASCTs, is generally recommended for those who do not achieve at least a very good partial response (VGPR) after the first ASCT, or those with high-risk features. The reason I found this interesting was that I faced a decision of single or tandem transplant in 2007.
The results of the study got very detailed for me but what I understood was important for the patient. Out of 12,763 patients, 6,581 underwent a single ASCT and 4,027 underwent tandem ASCT. Patients who received a second ASCT or an allogeneic transplant after the first six months of the initial ASCT were considered part of the single ASCT group. There was a shift in transplantation practices over time, with tandem ASCT becoming less common: 47.4% before 2008 versus 25.7% in 2017-2021. Moreover, the percentage of patients in complete remission (CR) post-induction therapy increased over time (7.4% between 1998-2007 versus 13% after 2017), as did the percentage achieving CR after the first ASCT (20.5% before 2008 vs. 32.3% after 2017).
When comparing single and tandem ASCTs, no significant difference in OS or EFS was observed for patients who achieved CR after the first transplant. However, patients who did not achieve CR after the first ASCT experienced a significant OS benefit with tandem ASCT. This benefit was also evident in patients who did not reach CR after induction therapy. Interestingly, there was no significant difference in OS or EFS for patients who transitioned from non-CR to CR after the first ASCT. The study analyzed the impact of the International Staging System (ISS) and renal impairment on outcomes. ISS stage III was significantly associated with worse OS for patients with renal impairment. Notably, patients with ISS stage I and no renal impairment showed a significant benefit in OS from tandem ASCT, while those with ISS stage III and renal impairment fared better with single ASCT.
Conclusion
Don’t ask me to explain much more than my current thoughts but the study shows that patients who did not achieve CR after induction therapy or the first ASCT benefited from a second ASCT. However, patients with ISS stage III and renal impairment had poorer outcomes, and in these cases, single ASCT was associated with better survival. What I liked about the study was these findings suggest a need for tailored approaches based on patient characteristics to optimize treatment strategies for NDMM patients. And I believe that is a good thing for the patient.
I recently took a deep dive into some of the scientific abstracts from the ASH conference, and let me tell you, it was like entering a different universe, one where genes, mutations, and complex terms I had never heard of were flying at me left and right. As someone who’s been living with multiple myeloma (MM), I wanted to better understand the cutting-edge research and what it means for us patients. While I can’t claim to fully comprehend everything I read (many of the abstracts went way over my head), one thing became very clear: the disease MM is a bit like a shapeshifter. And when reading the research abstracts slowly and methodically one can pull out one consistent thread…each genomic mutation/variation/depletion/gain is being closely looked at and evaluated to see how they can be interpreted and manipulated to achieve better outcomes for MM patients!
After reading through it slowly, I could piece together that the Sialyltransferase Gene (ST3GAL1) seems to play a role in MM progression. Specifically, increased expression of this gene is linked to a higher risk of relapse and lower progression-free survival. In other words, it’s one of those genetic markers that can predict how well a patient might do in the long term after treatment. The paper suggests that investigating desialylation strategies, or ways to reverse the effects of this gene, could be a promising area for future research. To a patient, this is incredibly encouraging! Not only are scientists working on new treatments, but they’re also looking at how to make current treatments work longer and more effectively.
The intensity and depth of this research is mind-boggling, and as stated above, although I can’t pretend to fully understand all the complexities of this research, I’m filled with hope. Every gene, mutation, and variation being studied is a potential pathway to better treatments for those of us living with multiple myeloma. So, while it may seem daunting to dive into these abstracts, I encourage my fellow patients to take a closer look. The future is full of promise, and the breakthroughs on the horizon could very well lead to a world where MM is no longer as unpredictable or devastating.
One of my highlights on Sunday at ASH 2024 was attending the session by Janine Joseph, MS, MBA. The title was, “Six-Month Resistance Training Interventions Are Associated with Improvements in Fatigue and Pain in Multiple Myeloma Patients.”
Because most patients experience some physical problems, I truly wanted to learn more.
This study explores the impact of different physical exercise (PE) interventions on the quality of life (QOL) of patients with multiple myeloma (MM), focusing on fatigue, pain, depression, and anxiety. Despite concerns about MM-related bone disease, the study confirms that PE, including resistance training (RT) and walking (W), can be safe and beneficial for MM patients.
The objective of the study was aimed to assess the effects of PE on QOL in MM patients, including specific symptoms like fatigue, pain, depression, and anxiety. The participants: MM patients enrolled in either a 6-month pilot intervention (supervised in-person RT group: unsupervised home-based W group or a 6-month remotely supervised RT intervention.) Quality-of-life assessments were done at three time points—baseline, end of intervention, and 6 months post-intervention.
The results were favorable. Fatigue improved during the intervention, particularly in the RT groups, but this improvement was lost post-intervention. Notably, after the intervention, there were increases in reported energy loss, feeling slowed down, and sleep problems. Pain improved in the supervised RT group during the intervention, with a significant reduction in visual analog scale (VAS) score, and these improvements persisted after the intervention. Depression did not show any significant changes in any of the groups throughout the study period. Anxiety worsened in the combined sample during the intervention, with the W group showing a notable decline. However, the changes in anxiety did not reach statistical significance, and it remains unclear if the anxiety change was related to the intervention or other factors. This may have been the result of a fear of injury.
The overall conclusion of the study is resistance training interventions are effective in improving fatigue and pain in MM patients, with sustained improvements in pain even after the intervention. Fatigue improvements were not sustained post-intervention, highlighting a potential area for further investigation into how to maintain such improvements long-term.
Anxiety showed a slight increase in the W group, but the cause of this increase remains uncertain. This was alarming to me since I am a former runner and currently a serious walker. Overall, RT interventions support physical QOL in MM patients, and further research is needed to explore how to sustain these benefits.
This analysis contributes valuable insights into how exercise interventions can support QOL in MM patients and underscores the need for additional strategies to help maintain long-term benefits.
I hope this has been helpful to you. The value of being as healthy as possible with MM is what I heard during the question and answer following the presentation. So much to learn and absorb. More to come later.
For the past four years, I’ve been part of the IMF’s ASH team, and during my first three years, I had the privilege of working alongside Jack Aiello. Jack was an extraordinary individual—a 29-year myeloma survivor and a relentless advocate for the myeloma community. His contributions to the ASH team were invaluable, and I found myself not only absorbing his insights but also learning from the grace and dedication he brought to this role. He was, in every sense, a role model to many of us on the team.
Jack’s final ASH blog was a numbered summary of key presentations—a format that reflected his clarity and commitment. As I write my final blog, I’m adopting his approach, both in tribute to him and in gratitude for all he taught me.
We miss you, Jack. Rest in peace, good man.
Most impactful abstracts related to smoldering myeloma treatments:
AQUILA PROSPECTIVE STUDY
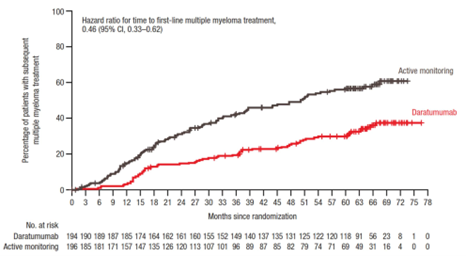
Aquila is a large (n=390) prospective study, initiated in late 2017, that randomized those with HRSMM into a treatment arm (daratumumab monotherapy, aka dara) and a control arm (observation). The goal is to determine the impact of early intervention with dara on the prevention of end-organ damage and the progression to active myeloma. The primary endpoint is progression (via CRAB or SLiMCRAB), with secondary endpoints of overall response rate (ORR), time to the first line of treatment, PFS on first line of treatment for active myeloma, and overall survival. While this was designed for HRSMM, applying the Mayo 2018 20-2-20 criteria retrospectively, the study included low-risk (20%), intermediate-risk (40%), and high-risk individuals (40%). The dara arm saw reduced risk of progression to active myeloma or death by 51%, and the ORR was 63.4%. The median time to first-line treatment was 50.2 months in the control arm, and the median is not yet reached in the dara arm. Health-related quality of life was maintained while on dara, with discontinuation in the study due to adverse events in the dara group being low, at 6.7%. Treatment-emergent adverse events (TEAEs) were low overall; the dara arm had 56 reports (29% of subjects) while the control arm had 38 reports (19%). Also, pneumonia was observed in 7 of the dara arm participants and 1 of the control arm participants. Grade 3 or 4 infections were also observed in 16% of dara participants and 4.6% of control arm participants, with infections lasting almost twice as long for those on dara. (Dimopoulos, 773)
My Thoughts on the AQUILA STUDY:
This abstract generated a lot of excitement, both during the conference and following. The results are encouraging, but I’m a bit more cautious than excited. I think these findings provide the opportunity for more questions. Participants in the dara arm still progressed to active treatment, albeit at a lower rate than the observation arm (see graph below). However, if the drug was truly effective, wouldn’t the rate to progression be much lower? Also, given that the risk stratification ended up having more high-risk individuals in the observation arm (43.9% versus 37.1% in dara arm) and fewer low risk (17.3% in observation arm versus 23.2% in the dara arm) once the 20-2-20 criteria were applied, the two groups might have had some differences that made an impact in these findings.
I also think this study needs more follow-up to determine the overall impact. Overall survival was highlighted as being better in the dara arm, however, I think more data and explanation are needed as typically people don’t die from smoldering myeloma, so what did the people in the observation arm pass away from? More granular analysis would be helpful. Admittedly, very detailed information is difficult to provide in a 12-minute presentation, and further updates on this study will help to fill in questions that I still have.
HOVON 147
HOVON147 explored carfilzomib-lenalidomide-dexamethasone (KRd) versus lenalidomide-dexamethasone (Rd) in those with high-risk smoldering multiple myeloma (HRSMM). This study began in 2016, so high-risk was identified by Pethema or Mayo 2008 criteria. Using Pethema, 94.7% were high-risk, using Mayo 2008, 10.5% were high-risk, and after Mayo 20-2-20 was developed, they looked back at the number that would have been classified as high risk according to that criteria, and that was 35%. After nine cycles, MRD negativity was 5% in the Rd arm and 57% in the KRd arm. At three years, the progression-free survival (PFS) was 94% for KRd and 40% for Rd. Progression to active myeloma occurred in 18% of those on the Rd arm and 6% on the KRd arm. Overall response rate (ORR) after nine cycles was 68% in the Rd arm and 97% in the KRd arm. Two deaths occurred within the Rd arm (progression to secondary plasma cell leukemia and cardiovascular event). Safety data showed issues with both arms, with more grade 3 events in the KRd arm (74%) than the Rd arm (48%). In the Rd arm, 35% of the participants completed the study, while 52% in the KRd completed the study. (Broijl, 676)
My Thoughts on Hovon 147
this study also possibly offers some exciting possibilities for the future. This phase 2 study has a relatively small sample size (n=58), which may affect generalizability. I also think that longer follow-up is needed to assess overall survival benefits and to monitor for relapsed/refractory status and/or other potential long-term effects.
CAR-PRISM Study
CAR-PRISM was a very small study examining the effectiveness, tolerability, and safety of CAR-T (cilta-cel) in those with HRSMM. Previous studies have suggested that using cilta-cel earlier in the treatment line leads to better outcomes. The immune microenvironment changes as the disease progresses, and perhaps better outcomes will result with the immune microenvironment is more fit (i.e., earlier in the disease pathway). One rationale for this study was to avoid exposure to SOC induction therapies and their associated toxicities. Total number in study is 20, but this presentation focused on the first six, who were included in the safety run-in. The primary endpoint is safety, and secondary endpoints include ORR, CR, MRD negativity, and PFS, as well as incidence and severity of AEs. All six experienced some cytokine release syndrome, four with grade one and two with grade two. No grade three or greater CRS. One experienced grade one Bell’s palsy that was resolved within two weeks, another experienced grade four immune related thrombocytopenia, also resolved within two weeks, one patient experienced transient grade three AST/ALT elevation, which was resolved. To date, there have been no grade three infections and no secondary malignancies. The median follow-up time for this data is 10.5 months. All six experienced an overall response rate of 100%, with all being complete responses. The MRD negative rate is 100%, as well. Three individuals have had their one-year follow up, and have sustained MRD negativity. None have developed biochemical or SLIM-CRAB progression to date. The study is on-going, and while these initial results are promising, the authors concluded that longer follow-up is needed to determine durability of response and help inform the risk and benefits of early use of cilta-cel in HRSMM. (Nadeem, 1027)
My Thoughts on the CAR-PRISM Study
Of the three studies, the outcomes of this study are the most exciting to me. I recognize the small sample size, but the findings seem quite positive. Like the other studies, more time to see how these individuals do (e.g., 3 years, 5 years, 10 years, etc…) is required. My concern with this study is its lack of transferability to the real world. CAR-T is expensive (over $2 million), and I doubt that many insurance plans will cover CAR-T for people who are asymptomatic.
Alternative approaches to delaying/preventing progression
Nutrivention Trial
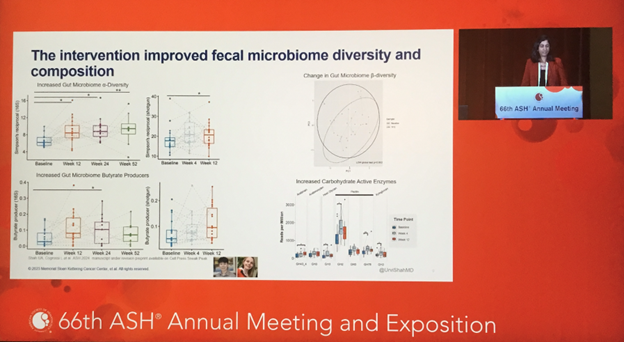
The Nutrivention trial explored whether a high-fiber, plant-based diet could delay the progression of myeloma precursor conditions (MGUS and SMM) to active myeloma. Twenty participants with a BMI ≥ 25 followed the diet for 12 weeks, eating to satiety without calorie restriction. Feasibility was demonstrated, with patients reporting improved quality of life and minimal difficulty adhering to the diet. Four participants discontinued medications, saving an average of $65 per month. Disease progression slowed in two patients, while others showed stable disease or lacked sufficient baseline data. The diet improved fecal microbiome diversity, reduced inflammation, and enhanced anti-tumor immunity, with these benefits correlating with BMI and dietary measures. Mouse model data supported the findings, showing delayed disease progression independent of calorie restriction. The study concluded that a high-fiber, plant-based diet could potentially slow MGUS and SMM progression. (Shah, 671)
My Thoughts on the Nutrivention Trial
The evidence continues to accumulate that lifestyle factors, including diet, may impact progression. One mechanism involves butyrate – a beneficial compound produced by gut bacteria and suspected to have anti-cancer and anti-inflammatory properties. It’s suggested that a whole-food, plant-based diet might increase butyrate (see slide capture below), potentially lowering the risk of disease progression.
Examining the psychological impacts of precursor conditions:
UK-Based Study on Precursor Diagnosis
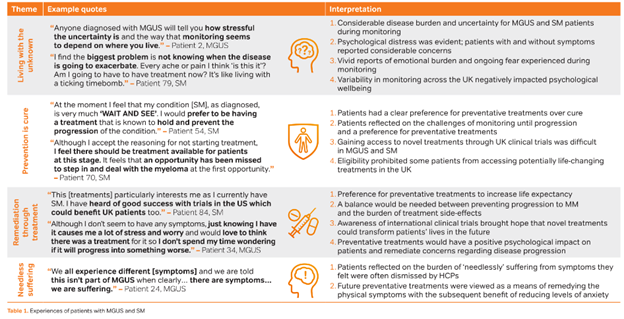
A UK-based study examined the psychological impacts of being diagnosed with a precursor condition. Using a mixed-methods approach, meaning collecting both quantitative and qualitative data, they found that with quality of life, those with MGUS and those with SMM has significantly worse scores than norms (based on general population), with MGUS people scoring a bit worse than those with SMM. Based on interviews, the researchers developed four themes from the qualitative data: (a) living with the unknown, (b) prevention is cure, (c) remediation through treatment, and (d) needless suffering. Some sample quotes and interpretation of these are included in the image below from the poster presentation.
This study is the first to assess racial disparities in cancer-related stress among patients undergoing active observation for indolent blood cancers (i.e., smoldering myeloma, lymphoma, CLL/SLL, etc; 14.6% of the sample had smoldering myeloma). The findings show that while ethnic minorities report similar levels of cancer-related stress when compared to non-Hispanic White patients, they often experience heightened fear and fatalism regarding cancer, which can foster beliefs that cancer development is uncontrollable and inevitably fatal. Such fatalistic views may deter engagement in preventative health behaviors and contribute to poorer health outcomes and harmful coping mechanisms, such as smoking. To mitigate these effects, targeted educational and psychological interventions are needed to address and reshape fatalistic beliefs about cancer in racially minoritized populations with indolent blood cancers. (Sklarz, 3739)
My Thoughts on the Study on Precursor Conditions
Understanding the psychological impact of living with precursor conditions like MGUS and SMM is crucial for improving patient care. The UK-based study highlights that individuals with these conditions often face significant reductions in quality of life, grappling with themes such as the uncertainty of disease progression, the hope of prevention, and concerns about needless suffering. Additionally, the first study on racial disparities in cancer-related stress reveals that while stress levels may not differ significantly between racial groups, ethnic minorities often carry heightened fears and fatalistic views about cancer. These beliefs can hinder engagement in preventative health measures and lead to poorer health outcomes. Addressing these psychological challenges through targeted education, counseling, and support interventions can empower patients to manage their condition more effectively and improve their overall well-being.
Study Introducing the PANGEA 2.0 Trajectory
This study introduces the PANGEA 2.0 trajectory model, designed to predict progression risk in smoldering multiple myeloma (SMM) with improved accuracy. Trained on over 1,000 patients and validated on a multi-center cohort of over 100 patients with longitudinal follow-up, the model detects early progression patterns and remains robust even without prior lab results. An easy-to-use online calculator will soon be available, though further validation with new cohorts and integrated FISH results is planned. (Chabrun, 1017)
Study on Heterogeneity Within SMM
This study highlights the heterogeneity within smoldering multiple myeloma (SMM), suggesting the presence of MM-like SMM and MGUS-like SMM that are currently grouped together under existing criteria. Differentiating these subtypes could improve clinical decision-making and trial design, with genomic data playing a critical role in refining classifications and defining myeloma progression events. (Samur, 1018)
Study Using Whole-Genome Sequencing to Predict Tumor Progression in Precancerous Stages of MM
This study demonstrates that whole-genome sequencing (WGS) and the MM-like score can predict tumor progression from precancerous stages, placing tumors on a continuum toward multiple myeloma (MM). The MM-like score, derived from clinically available WGS, identifies driver mutations, tracks subclone evolution, and informs disease risk, with findings suggesting MM may begin decades before diagnosis. Future research will assess the impact of these insights on IMWG recommendations and clinical practice. (Alberge, 1019)
Study on Using Circulating Tumor Cells As a Biomarker for Monitoring Myeloma
Circulating tumor cells (CTCs) are detectable in 35.6% of patients with asymptomatic monoclonal gammopathies (SMM, 54%; MGUS, 22%) and are linked to higher progression risk in SMM. While further follow-up is needed to clarify their role in MGUS and additive value over existing risk tools, CTCs show promise as a non-invasive biomarker for monitoring disease evolution longitudinally. (Malandrakis, 1020)
Study on Imaging Techniques in Myeloma After 2014
This study examines the risk and patterns of progression in smoldering multiple myeloma (SMM) diagnosed after 2014, when advanced imaging became routine. Progression events predominantly involved anemia, SLiM criteria, or asymptomatic bone disease detected during routine imaging. Patients classified as low or intermediate risk per the 20-2-20 score or low risk by the IMWG tool showed low progression rates similar to MGUS. High-risk SMM cases had lower progression risks than earlier cohorts, likely due to advanced imaging at diagnosis. While the IMWG tool may better identify intermediate/high-risk patients, it categorizes only a small group. Advanced imaging helps reassure low-risk patients of their favorable prognosis, and for high-risk individuals, clinical trials should be prioritized without overtreatment based solely on current tools. (Kastritis, 4675)
Conclusion
In closing, the advancements presented at this year’s ASH meeting reflect the remarkable strides being made in our understanding and treatment of smoldering myeloma. From innovative treatment strategies and understanding the psychological impacts on those living with these diagnoses to groundbreaking scientific insights into disease progression, this work brings closer to a more personalized and hopeful approach to care. These achievements would not be possible without the tireless efforts of the researchers, the support of the IMF, our generous sponsors, and the collaboration of my incredible ASH teammates. Thank you to everyone! That’s an ASH wrap!
One of the most relevant sessions for those interested in smoldering myeloma was a Spotlight Session called “Smoldering Myeloma: A Case for Early Intervention?” presented by Maria-Victoria Mateos, MD, PhD, and Karthik Ramasamy, MD, PhD. The seventy-five-minute session featured a two-sided debate on whether early intervention is appropriate for smoldering myeloma. Dr. Mateos argued in favor of early intervention, while Dr. Ramasamy presented the opposing perspective.
Before presenting their arguments, important points about diagnosing and monitoring SMM were emphasized:
Rule out other conditions: Diseases like diabetes, hypertension, and vitamin deficiencies can mimic signs of myeloma.
Confirm the diagnosis: Doctors should check for the presence of the M-protein. They should also ensure there is no anemia, kidney issues, or high calcium levels, and repeat these tests at least once to confirm stability.
Conduct a full evaluation: Tests like free light chain (FLC) assessment, MRI, and bone marrow biopsy help ensure no active myeloma-defining events (MDEs) are present.
Assessing the risk of SMM progressing to active myeloma is critical for providing the right care. Risk models estimate the chance of progression, typically identifying patients with a 50% risk of developing myeloma within two years. Ideal models combine clinical, biological, and dynamic markers. Examples include:
The Pethema model
Bence Jones proteinuria (protein in urine)
Evolving M-spike patterns or changes in M-spike and hemoglobin levels
PET-CT imaging
The PANGEA model
(Note: The “20-2-20” model, widely used in the U.S., was not presented.)
Dr. Mateos began with the question, “Smoldering Myeloma: A case for early intervention?” Her position was clear: early treatment offers the best chance to cure myeloma. However, she noted that “cure” must be carefully defined. She referenced a 1963 definition of cure: after a decade or two, patients are disease-free and have a similar life expectancy to the general population.
She outlined the challenges of achieving a cure:
Myeloma is a complex and diverse disease, not a single condition.
Treatment should be personalized: frail patients or those with high-risk features need different approaches than fit, low-risk, or asymptomatic individuals.
Dr. Mateos supported her argument with studies showing promising results for early treatment:
Aquila study
GEM-CESAR trial
ASCENT trial
Immuno-PRISM and CAR-PRISM studies
She concluded:
Results from these studies are encouraging, but they need longer follow-up to confirm if early treatment leads to a lasting cure.
Treating high-risk SMM (HR-SMM) with therapies used in active myeloma may offer a curative option.
Patients with newly diagnosed myeloma (NDMM) and no high-risk features may also achieve cure-like outcomes.
A key point here is that the main difference between HR-SMM and NDMM is the absence of myeloma-defining events (MDEs) in HRSMM.
Dr. Ramasamy countered Dr. Mateos’ position by stating: “Early intervention only adds costs and toxicity unless we treat the right patient, at the right time, with the right goal.”
He highlighted the complexities of SMM:
Myeloma remains incurable despite advances.
SMM is a heterogeneous disease—not all patients progress in the same way.
Patients have different priorities and expectations for treatment.
Effective therapies already exist to treat active myeloma, and earlier use can be studied further.
SMM is a large population—how many patients would truly benefit from early treatment?
Dr. Ramasamy then asked: “Under what conditions is early intervention valid?” He proposed five criteria:
SMM cells are sensitive to treatment.
Treatment happens before the disease evolves further.
Treatment is tailored to individual patients.
Early intervention prevents life-altering complications during monitoring.
Early treatment improves survival.
He compared SMM and NDMM studies to examine treatment response:
In transplant-eligible patients, response rates (VGPR or better) were similar for SMM and NDMM.
In transplant-ineligible patients, NDMM studies showed better responses than SMM studies.
Dr. Ramasamy then laid out the pros and cons of treatment approaches in SMM. The following table is a reproduction of one of his slides:
Prevent/Delay Active Myeloma
Functionality Cure Myeloma
Pros
Low-intensity approach Relatively fewer side effects Applicable to the majority of SMM patients
High potential for treatment-free period Deep responses
Cons
May require further therapy Lower response rate Lack of deep responses
High-intensity approach Higher risk of adverse events Applicable for a smaller proportion of patients Risk of multidrug resistant clones
Dr. Ramasamy pointed out challenges with current SMM trials:
Changing definitions of high-risk SMM (HRSMM) and NDMM complicate results (e.g., SLiM CRAB criteria, Mayo “20-2-20,” and IMWG criteria).
Lack of survival data: Only the DETER-SMM trial measures overall survival as an outcome.
Toxicity concerns: Some trials report side effects and reduced quality of life for patients receiving early treatment.
Dr. Ramasamy suggested next steps:
Better monitoring tools: Improve risk models, use whole-body MRI for imaging, and follow care standards.
Patient involvement: Include patient preferences in research, explore barriers to treatment, and set toxicity limits in trials.
Refine treatment approaches: Develop personalized treatments tailored to individual patients.
Cost-effective therapies: Recognize the financial burden on patients, including treatment costs, managing side effects, and lost productivity.
Dr. Ramasamy’s final points included the following:
Enhance monitoring tools alongside early treatment models.
Prioritize patient involvement in research.
Focus early treatment trials on patients at the highest risk of progression.
Design trials to reduce short- and long-term side effects.
Develop affordable treatment strategies to maximize accessibility.
Conclusion
The debate between Drs. Mateos and Ramasamy highlighted the uncertainties surrounding early intervention for SMM. Mateos argued that early treatment offers hope for a cure, especially for high-risk patients, while Ramasamy emphasized caution, patient priorities, and the need for refined, cost-effective approaches.
For those with SMM, it’s essential to carefully consider the risks and benefits of early treatment. Discuss all options with your doctor, evaluate your personal risk tolerance, and consider your long-term goals before making a decision. Research is advancing, but there are still more questions than answers in this complex space.
The 66th annual American Society of Hematology (ASH) meeting again did not disappoint. Approximately 30,000 people (Health care professionals, pharmaceutical representatives, researchers, and others converged on San Diego, CA, for this premier meeting. I was able to attend many key oral abstracts and education programs related to multiple myeloma. The presentations came like a firehose of information.
Information related to real-world experience, enhancing patient quality of life, and addressing frailty continues to be highlighted at an increasing volume.
Smoldering myeloma continues to be an area of controversy about whether to treat or not treat. However, results from the Aquila trial seem to be leading us in the direction of early treatment for high risk smoldering myeloma.
Advances continue to be made not only in myeloma therapy, but in other domains of the myeloma experience like supportive care and identifying testing that may direct treatment decision-making
Dr. Joseph Mikhael, IMF Chief Medical Officer, will be joined by Beth Faiman, PhD, Nikhil Munshi, MD and Vincent Rajkumar, MD, and will discuss advances in myeloma research from the 2024 ASH Conference.
These and other great events are being planned, including the 2025 Patient and Family Seminars and Regional Community Workshops. Find these and more at Myeloma.org/events.
I want to extend my gratitude to:
The IMF for continuing to include me in this amazing program, Myeloma Voices, where the patient voice is shared through social media to provide updates on myeloma data that impacts those living with this diagnosis. It is a privilege and an honor to attend with this group who volunteers their time to help others living with myeloma.
Our sponsors of Myeloma Voices: Johnson & Johnson, Regeneron, and Karyopharm Therapeutics. Your support of myeloma patients’ learning is much appreciated.
The IMF Meetings and Support Group Teams for all that you do to make this program happen. So many details that others will never know because you do it seamlessly and make it look easy.
The Myeloma Voices, both virtual and in person. You volunteer your time, work through complex information and long schedules to attend the sessions, and share your experiences with your followers.
You can see how visible some of the leaders were at #ASH24, making the Social Media Leaderboard!
You can continue to follow these folks on social media and learn more about #ASH24 and other #myeloma happenings.
Sheri Baker @blondie1746 Yelak Biru @NorthTxMSG Becky Bosley @MidAtlanticMSG Barbara Davis @bkinoglu Jessie Daw @Daw6Jessie Oya Gilbert @HHHHFoundation Terry Glassman @TerryGlassman Linda Huguelet @LindaMyeloma Teresa Miceli @IMFnurseMyeloma Rob Salmon @salmon_rob Jim Shoemaker @JimJhs17 Michael Tuohy @IMFmikeMYELOMA Robin Tuohy @IMFsupport Jenn Wieworka @jwiework Jill Zitzewitz @JillZitzewitz
Search social media for key hashtags: #MMSM #Myeloma #ASH24 #IMFASH24
My best, Teresa Miceli, RN BSN OCN Myeloma Voices Nurse Liaison Support Group Leader IMF Nurse Leadership Board