ASH Summary on Smoldering Multiple Myeloma (SMM)
For the past four years, I’ve been part of the IMF’s ASH team, and during my first three years, I had the privilege of working alongside Jack Aiello. Jack was an extraordinary individual—a 29-year myeloma survivor and a relentless advocate for the myeloma community. His contributions to the ASH team were invaluable, and I found myself not only absorbing his insights but also learning from the grace and dedication he brought to this role. He was, in every sense, a role model to many of us on the team.
Jack’s final ASH blog was a numbered summary of key presentations—a format that reflected his clarity and commitment. As I write my final blog, I’m adopting his approach, both in tribute to him and in gratitude for all he taught me.
We miss you, Jack. Rest in peace, good man.

Most impactful abstracts related to smoldering myeloma treatments:
AQUILA PROSPECTIVE STUDY
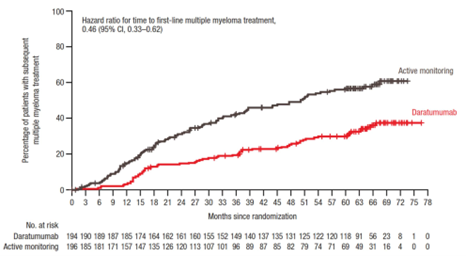
Aquila is a large (n=390) prospective study, initiated in late 2017, that randomized those with HRSMM into a treatment arm (daratumumab monotherapy, aka dara) and a control arm (observation). The goal is to determine the impact of early intervention with dara on the prevention of end-organ damage and the progression to active myeloma. The primary endpoint is progression (via CRAB or SLiMCRAB), with secondary endpoints of overall response rate (ORR), time to the first line of treatment, PFS on first line of treatment for active myeloma, and overall survival. While this was designed for HRSMM, applying the Mayo 2018 20-2-20 criteria retrospectively, the study included low-risk (20%), intermediate-risk (40%), and high-risk individuals (40%). The dara arm saw reduced risk of progression to active myeloma or death by 51%, and the ORR was 63.4%. The median time to first-line treatment was 50.2 months in the control arm, and the median is not yet reached in the dara arm. Health-related quality of life was maintained while on dara, with discontinuation in the study due to adverse events in the dara group being low, at 6.7%. Treatment-emergent adverse events (TEAEs) were low overall; the dara arm had 56 reports (29% of subjects) while the control arm had 38 reports (19%). Also, pneumonia was observed in 7 of the dara arm participants and 1 of the control arm participants. Grade 3 or 4 infections were also observed in 16% of dara participants and 4.6% of control arm participants, with infections lasting almost twice as long for those on dara. (Dimopoulos, 773)
My Thoughts on the AQUILA STUDY:
This abstract generated a lot of excitement, both during the conference and following. The results are encouraging, but I’m a bit more cautious than excited. I think these findings provide the opportunity for more questions. Participants in the dara arm still progressed to active treatment, albeit at a lower rate than the observation arm (see graph below). However, if the drug was truly effective, wouldn’t the rate to progression be much lower? Also, given that the risk stratification ended up having more high-risk individuals in the observation arm (43.9% versus 37.1% in dara arm) and fewer low risk (17.3% in observation arm versus 23.2% in the dara arm) once the 20-2-20 criteria were applied, the two groups might have had some differences that made an impact in these findings.
I also think this study needs more follow-up to determine the overall impact. Overall survival was highlighted as being better in the dara arm, however, I think more data and explanation are needed as typically people don’t die from smoldering myeloma, so what did the people in the observation arm pass away from? More granular analysis would be helpful. Admittedly, very detailed information is difficult to provide in a 12-minute presentation, and further updates on this study will help to fill in questions that I still have.
HOVON 147
HOVON147 explored carfilzomib-lenalidomide-dexamethasone (KRd) versus lenalidomide-dexamethasone (Rd) in those with high-risk smoldering multiple myeloma (HRSMM). This study began in 2016, so high-risk was identified by Pethema or Mayo 2008 criteria. Using Pethema, 94.7% were high-risk, using Mayo 2008, 10.5% were high-risk, and after Mayo 20-2-20 was developed, they looked back at the number that would have been classified as high risk according to that criteria, and that was 35%. After nine cycles, MRD negativity was 5% in the Rd arm and 57% in the KRd arm. At three years, the progression-free survival (PFS) was 94% for KRd and 40% for Rd. Progression to active myeloma occurred in 18% of those on the Rd arm and 6% on the KRd arm. Overall response rate (ORR) after nine cycles was 68% in the Rd arm and 97% in the KRd arm. Two deaths occurred within the Rd arm (progression to secondary plasma cell leukemia and cardiovascular event). Safety data showed issues with both arms, with more grade 3 events in the KRd arm (74%) than the Rd arm (48%). In the Rd arm, 35% of the participants completed the study, while 52% in the KRd completed the study. (Broijl, 676)
My Thoughts on Hovon 147
this study also possibly offers some exciting possibilities for the future. This phase 2 study has a relatively small sample size (n=58), which may affect generalizability. I also think that longer follow-up is needed to assess overall survival benefits and to monitor for relapsed/refractory status and/or other potential long-term effects.
CAR-PRISM Study
CAR-PRISM was a very small study examining the effectiveness, tolerability, and safety of CAR-T (cilta-cel) in those with HRSMM. Previous studies have suggested that using cilta-cel earlier in the treatment line leads to better outcomes. The immune microenvironment changes as the disease progresses, and perhaps better outcomes will result with the immune microenvironment is more fit (i.e., earlier in the disease pathway). One rationale for this study was to avoid exposure to SOC induction therapies and their associated toxicities. Total number in study is 20, but this presentation focused on the first six, who were included in the safety run-in. The primary endpoint is safety, and secondary endpoints include ORR, CR, MRD negativity, and PFS, as well as incidence and severity of AEs. All six experienced some cytokine release syndrome, four with grade one and two with grade two. No grade three or greater CRS. One experienced grade one Bell’s palsy that was resolved within two weeks, another experienced grade four immune related thrombocytopenia, also resolved within two weeks, one patient experienced transient grade three AST/ALT elevation, which was resolved. To date, there have been no grade three infections and no secondary malignancies. The median follow-up time for this data is 10.5 months. All six experienced an overall response rate of 100%, with all being complete responses. The MRD negative rate is 100%, as well. Three individuals have had their one-year follow up, and have sustained MRD negativity. None have developed biochemical or SLIM-CRAB progression to date. The study is on-going, and while these initial results are promising, the authors concluded that longer follow-up is needed to determine durability of response and help inform the risk and benefits of early use of cilta-cel in HRSMM. (Nadeem, 1027)
My Thoughts on the CAR-PRISM Study
Of the three studies, the outcomes of this study are the most exciting to me. I recognize the small sample size, but the findings seem quite positive. Like the other studies, more time to see how these individuals do (e.g., 3 years, 5 years, 10 years, etc…) is required. My concern with this study is its lack of transferability to the real world. CAR-T is expensive (over $2 million), and I doubt that many insurance plans will cover CAR-T for people who are asymptomatic.
Alternative approaches to delaying/preventing progression
Nutrivention Trial
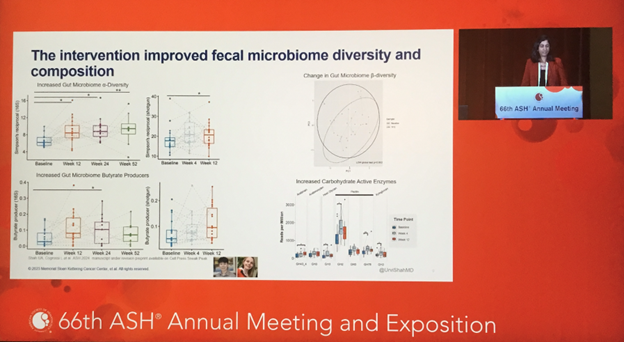
The Nutrivention trial explored whether a high-fiber, plant-based diet could delay the progression of myeloma precursor conditions (MGUS and SMM) to active myeloma. Twenty participants with a BMI ≥ 25 followed the diet for 12 weeks, eating to satiety without calorie restriction. Feasibility was demonstrated, with patients reporting improved quality of life and minimal difficulty adhering to the diet. Four participants discontinued medications, saving an average of $65 per month. Disease progression slowed in two patients, while others showed stable disease or lacked sufficient baseline data. The diet improved fecal microbiome diversity, reduced inflammation, and enhanced anti-tumor immunity, with these benefits correlating with BMI and dietary measures. Mouse model data supported the findings, showing delayed disease progression independent of calorie restriction. The study concluded that a high-fiber, plant-based diet could potentially slow MGUS and SMM progression. (Shah, 671)
My Thoughts on the Nutrivention Trial
The evidence continues to accumulate that lifestyle factors, including diet, may impact progression. One mechanism involves butyrate – a beneficial compound produced by gut bacteria and suspected to have anti-cancer and anti-inflammatory properties. It’s suggested that a whole-food, plant-based diet might increase butyrate (see slide capture below), potentially lowering the risk of disease progression.
Examining the psychological impacts of precursor conditions:
UK-Based Study on Precursor Diagnosis
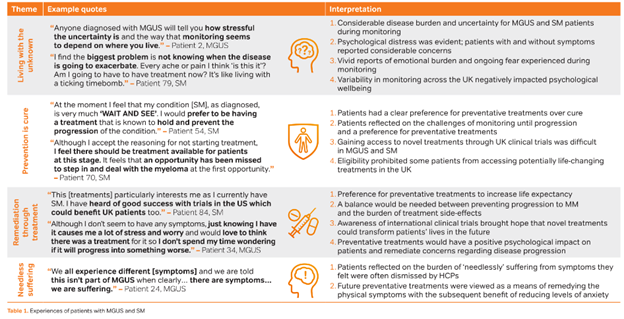
A UK-based study examined the psychological impacts of being diagnosed with a precursor condition. Using a mixed-methods approach, meaning collecting both quantitative and qualitative data, they found that with quality of life, those with MGUS and those with SMM has significantly worse scores than norms (based on general population), with MGUS people scoring a bit worse than those with SMM. Based on interviews, the researchers developed four themes from the qualitative data: (a) living with the unknown, (b) prevention is cure, (c) remediation through treatment, and (d) needless suffering. Some sample quotes and interpretation of these are included in the image below from the poster presentation.
This study is the first to assess racial disparities in cancer-related stress among patients undergoing active observation for indolent blood cancers (i.e., smoldering myeloma, lymphoma, CLL/SLL, etc; 14.6% of the sample had smoldering myeloma). The findings show that while ethnic minorities report similar levels of cancer-related stress when compared to non-Hispanic White patients, they often experience heightened fear and fatalism regarding cancer, which can foster beliefs that cancer development is uncontrollable and inevitably fatal. Such fatalistic views may deter engagement in preventative health behaviors and contribute to poorer health outcomes and harmful coping mechanisms, such as smoking. To mitigate these effects, targeted educational and psychological interventions are needed to address and reshape fatalistic beliefs about cancer in racially minoritized populations with indolent blood cancers. (Sklarz, 3739)
My Thoughts on the Study on Precursor Conditions
Understanding the psychological impact of living with precursor conditions like MGUS and SMM is crucial for improving patient care. The UK-based study highlights that individuals with these conditions often face significant reductions in quality of life, grappling with themes such as the uncertainty of disease progression, the hope of prevention, and concerns about needless suffering. Additionally, the first study on racial disparities in cancer-related stress reveals that while stress levels may not differ significantly between racial groups, ethnic minorities often carry heightened fears and fatalistic views about cancer. These beliefs can hinder engagement in preventative health measures and lead to poorer health outcomes. Addressing these psychological challenges through targeted education, counseling, and support interventions can empower patients to manage their condition more effectively and improve their overall well-being.
Study Introducing the PANGEA 2.0 Trajectory
This study introduces the PANGEA 2.0 trajectory model, designed to predict progression risk in smoldering multiple myeloma (SMM) with improved accuracy. Trained on over 1,000 patients and validated on a multi-center cohort of over 100 patients with longitudinal follow-up, the model detects early progression patterns and remains robust even without prior lab results. An easy-to-use online calculator will soon be available, though further validation with new cohorts and integrated FISH results is planned. (Chabrun, 1017)
Study on Heterogeneity Within SMM
This study highlights the heterogeneity within smoldering multiple myeloma (SMM), suggesting the presence of MM-like SMM and MGUS-like SMM that are currently grouped together under existing criteria. Differentiating these subtypes could improve clinical decision-making and trial design, with genomic data playing a critical role in refining classifications and defining myeloma progression events. (Samur, 1018)
Study Using Whole-Genome Sequencing to Predict Tumor Progression in Precancerous Stages of MM
This study demonstrates that whole-genome sequencing (WGS) and the MM-like score can predict tumor progression from precancerous stages, placing tumors on a continuum toward multiple myeloma (MM). The MM-like score, derived from clinically available WGS, identifies driver mutations, tracks subclone evolution, and informs disease risk, with findings suggesting MM may begin decades before diagnosis. Future research will assess the impact of these insights on IMWG recommendations and clinical practice. (Alberge, 1019)
Study on Using Circulating Tumor Cells As a Biomarker for Monitoring Myeloma
Circulating tumor cells (CTCs) are detectable in 35.6% of patients with asymptomatic monoclonal gammopathies (SMM, 54%; MGUS, 22%) and are linked to higher progression risk in SMM. While further follow-up is needed to clarify their role in MGUS and additive value over existing risk tools, CTCs show promise as a non-invasive biomarker for monitoring disease evolution longitudinally. (Malandrakis, 1020)
Study on Imaging Techniques in Myeloma After 2014
This study examines the risk and patterns of progression in smoldering multiple myeloma (SMM) diagnosed after 2014, when advanced imaging became routine. Progression events predominantly involved anemia, SLiM criteria, or asymptomatic bone disease detected during routine imaging. Patients classified as low or intermediate risk per the 20-2-20 score or low risk by the IMWG tool showed low progression rates similar to MGUS. High-risk SMM cases had lower progression risks than earlier cohorts, likely due to advanced imaging at diagnosis. While the IMWG tool may better identify intermediate/high-risk patients, it categorizes only a small group. Advanced imaging helps reassure low-risk patients of their favorable prognosis, and for high-risk individuals, clinical trials should be prioritized without overtreatment based solely on current tools. (Kastritis, 4675)
Conclusion
In closing, the advancements presented at this year’s ASH meeting reflect the remarkable strides being made in our understanding and treatment of smoldering myeloma. From innovative treatment strategies and understanding the psychological impacts on those living with these diagnoses to groundbreaking scientific insights into disease progression, this work brings closer to a more personalized and hopeful approach to care. These achievements would not be possible without the tireless efforts of the researchers, the support of the IMF, our generous sponsors, and the collaboration of my incredible ASH teammates. Thank you to everyone! That’s an ASH wrap!