Smoldering Myeloma at ASH 2024: What We’ve Learned So Far
The first two days of the 66th American Society of Hematology (ASH) Annual Meeting—Friday’s Satellite Symposium and Saturday’s research presentations—offered limited content specifically focused on smoldering myeloma (SMM). However, a few key discussions stood out, providing insights into treatment strategies, disease progression mechanisms, and the psychological impact of living with precursor conditions. These set the stage for additional abstracts on SMM during the rest of the conference.
Understanding Disease Progression: From MGUS to Myeloma
A presentation by Dr. Michaela Liedtke, MD, examined the mechanisms driving the progression of monoclonal gammopathy of undetermined significance (MGUS) to active myeloma. While the talk focused on MGUS, the findings are also relevant for SMM, which serves as an intermediate stage.
Dr. Liedtke categorized progression mechanisms into three main areas:
- Clone Intrinsic Factors: These include the type and level of the M-protein, abnormal light chain ratios, and specific genetic mutations.
- Clone-Host Interactions: The interplay between cancerous cells and the patient’s immune system or bone marrow microenvironment is critical in disease evolution.
- Host Factors: Patient-specific factors, like age and obesity, also influence disease progression.
These insights reinforce the importance of understanding individual risk profiles in managing precursor conditions like MGUS and SMM. Questions I have as someone with SMM include how can we significantly change our immune system function and/or the bone marrow microenvironment? Also, while I cannot control my age, I do have some measure of control over my body mass and fitness.
Treatment Decisions for Smoldering Myeloma
The transition from smoldering myeloma (SMM) to active myeloma is complex, and decisions about treatment are critical. In one of Friday’s Satellite Symposiums, Dr. Shaji Kumar, MD, presented on “Newly Diagnosed Multiple Myeloma: Many Choices and More Questions,” and this content has some relevance for those with SMM. As a reminder, the standard of care for low and intermediate-risk SMM is active surveillance, while for high-risk, it is either active surveillance or possible treatment, preferably within a clinical trial.
One of the key messages is that the first treatment can set the stage for long-term outcomes. Indeed, the goals of initial treatment were highlighted.
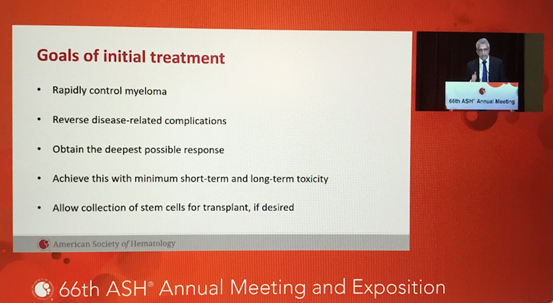
We want to use the very best treatment first, as we don’t want any subclones that remain and develop into treatment-resistant clones down the road. Dr. Kumar highlighted obtaining the deepest response possible, and I’ve heard other specialists emphasize that making the initial therapy the best possible choice can influence overall survival and quality of life.
Additionally, care must be tailored to each individual. Factors like genetic markers, disease aggressiveness, and a patient’s overall health (including frailty) play crucial roles in developing a treatment plan. Frailty in particular was highlighted as a major determinant of survival and should inform both treatment intensity and supportive care measures.
For those with SMM, this information is crucial, especially when deciding between active surveillance/watchful waiting, starting treatment, or participating in clinical trials. For me personally, I’ve decided to wait as long as possible to start treatment (I have three high-risk cytogenetic features), using the time instead to get in the best shape possible while eating the best foods possible.
The Psychological Toll of Precursor Conditions
Living with a precursor condition such as MGUS or SMM is not just a physical challenge—it’s a mental one, too. Interestingly, while some specialists have noted that their SMM patients experience higher levels of anxiety than those with active myeloma, studies on this topic have produced conflicting results.
At last year’s ASH, the iSTOPMM study reported minimal psychological impact associated with being diagnosed with a precursor condition. However, a UK-based study by Dr. Sandra Quinn, PhD, and colleagues presented at this year’s ASH found the opposite. Using both quantitative surveys and qualitative analysis, the study revealed that both MGUS and SMM patients experience reduced health-related quality of life (HRQoL) compared to the general population.
Key findings included:
- MGUS patients reported worse outcomes than SMM patients in areas like anxiety, depression, fatigue, and sleep disruption.
- Qualitative data highlighted themes such as:
- Living with the Unknown: The uncertainty of disease progression weighs heavily on patients.
- Prevention as Cure: Many patients feel they are constantly searching for ways to prevent disease progression.
- Remediation Through Treatment: Treatment is often seen as the only way to restore normalcy.
- Needless Suffering: Some patients feel trapped by the lack of clear guidelines for managing precursor conditions.
- This underscores the need for psychosocial support alongside clinical care to help patients navigate the emotional challenges of living with these conditions. Personally, I experienced significant anxiety in the first few years after my diagnosis. I’m more accepting of this now, and in a way, I look at this diagnosis as a gift as I’ve been given the opportunity to re-evaluate my life and how I’m living it. I think I needed some critical incident to make this happen, and I appreciate the changes I’ve made.
Final Thoughts
While the first two days of ASH 2024 offered limited SMM-specific content, these highlights provide valuable perspectives for patients and providers alike. The conference schedule suggests that Sunday, and especially Monday, will feature more in-depth discussions on smoldering myeloma. Stay tuned for additional updates as the conversation around SMM continues to evolve.