

Many Unique Data Points on the Myeloma Treatment Landscape
Friday is Satellite Symposia Day! It’s the day before the official meeting starts, when industry partners sponsor continuing medical education sessions for community treating physicians. I attended not 1, or 2, or even 3, but 4 of these sessions! I couldn’t resist. All the rockstars of the multiple myeloma world were presenting summaries of the latest treatment best practices. There are so many new clinical trials and recently FDA-approved myeloma therapies that are transforming outcomes for patients! The talks were interspersed with discussions, clinical cases, and quizzes on treatment options for the clinician audience. I was pleasantly surprised that I was able to answer nearly all the questions correctly! Being a patient advocate has taught me a lot, and it probably doesn’t hurt that I teach graduate and medical students at the academic medical center where I get my care.
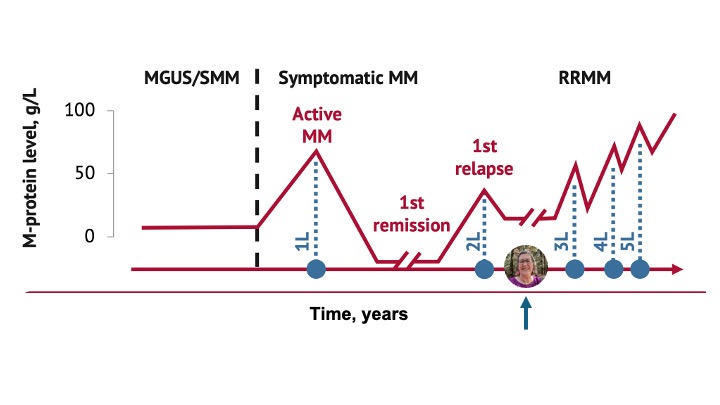
The common organizational structure of each of these symposia was to divide the talks by disease status, including discussions of newly diagnosed multiple myeloma (both transplant eligible or ineligible), first relapse, and then successive relapses in relapsed refractory myeloma (RRMM). There is often an image where myeloma disease status is plotted as a function of time, showing how patients respond to treatment in each line of therapy. It ends up looking a bit like a mountain range, and as a scientist, I love these plots. I studied protein folding throughout my career, and I made a lot of figures that looked quite similar. For fun, I took the liberty of adding myself as a data point to an image that was presented in the first session that I attended called “Bridging Gaps in Multiple Myeloma Care: A Community Oncologist’s Guide to Navigating the Evolving Treatment Landscape.” In this session, led by Drs. Caitlin Costello, MD; and Rahul Banerjee, MD, FACP; I learned that anti-CD38+ antibodies are the treating oncologist’s friend because they deepen the depth and length of response. It got me thinking about how I’ve been on my second line of therapy, Darzalex (daratumumab), Pomalyst (pomalidomide) and dexamethasone – DPd, for nearly 4 years now. I had my first relapse about 2 years after my stem cell transplant, but quad therapies were not even an option then. Who knows how long it will be before I need a third line of therapy? I’m sitting happily in that long break of time on the plot between relapses, enjoying every day!
The common theme for all of today’s sessions was that each patient is a unique case. Now that there are so many new therapies in the myeloma tool kit that have been FDA-approved, we are learning a lot about how they perform in the real world, with patients who wouldn’t have qualified for a clinical trial because of comorbidities or other challenges. It was encouraging to see that patient preferences and lifestyle choices are playing a key role in deciding next therapies, along with disease status and side-effect and treatment management. Additionally, each of today’s sessions also focused on unmet needs in access to care and how community oncologists can partner with myeloma specialists at academic medical centers to ensure that each patient gets the care that is right for them. It was encouraging to hear discussions of shared decision-making, fostering inclusiveness, and supporting patients’ priorities for their lives. Indeed, each myeloma patient is a unique data point on the evolving myeloma treatment landscape, and I find it so hopeful that we’re learning so much how to implement the right treatment option for each unique patient at different points in time so that they can enjoy a high quality of life.
Jill Zitzewitz, PhD, Central MA Multiple Myeloma Support Group
Follow me on X @JillZitzewitz